If you are here and still reading, thanks for being so patient! Our family has been very busy over the last six months, living, moving and preparing for Alexander's surgery in Boston on April 24th.
Alexander’s first 7 days of life was spent in the Intensive
Care Unit. He underwent several
diagnostic tests to better pinpoint his anatomy. On the morning of his 8th day, we
handed him helplessly to surgeons and hoped that he would survive. For 115 minutes his tiny heart did not beat,
his lungs did not breathe, his body was cold.
One-hundred fifteen minutes~nearly two hours~Alexander relied completely
on heart-lung bypass to ensure his body and mind could survive the repair to
his heart.
A newborn’s heart is about the size of a walnut. Because of this minuscule size, our surgical
team did not feel they could complete Alexander’s repair in one surgery,
however, it was vital to get his ventricles pumping to their appropriate
systems.
The ventricles (or lower chambers) are the muscles that pump
the blood to where it needs to go. They
are structurally different as the right normally pumps just to the lungs, and
the left pumps to the entire body. The
left ventricle is able to pump at high pressures for a very long time (a
lifetime!) and the right pumps at a much lower pressure as the blood only needs
to travel a short distance to the lungs.
With Alexander’s TGA (transposition of the great arteries)
his left lung was pumping to his lungs and the right to his body. Even though he had enough mixing of his
oxygenated and deoxygenated blood to keep his tissues reasonably oxygenated,
within just a few weeks, his left ventricle would start to atrophy, or weaken,
as it was not pumping to his body. In
the meantime, his lungs would be getting more pressure and blood than they were
intended and this would be bad for them as well. If you can imagine the lungs like a balloon,
but this balloon isn’t meant to be expanded endlessly, it is only meant to fill
just to capacity and empty. If it’s
stretched too much or too often, it becomes weaker, just like a real balloon.

This procedure, while straightforward on paper, takes
amazing precision as the great arteries are smaller than drinking straws and
the tiny coronary arteries (vessels that supply oxygen-rich blood to the heart)
are wire thin. Once, while marveling
with a nurse about the miracles these steady hands perform, she mentioned that
many of the suture threads are so light that they float instead of hang.
While he was in the operating room, they also ligated his
left-Superior Vena Cava (l-SVC), made repair to a Ventricular Septal Defect
(VSD), and performed an atrial septoctomy.
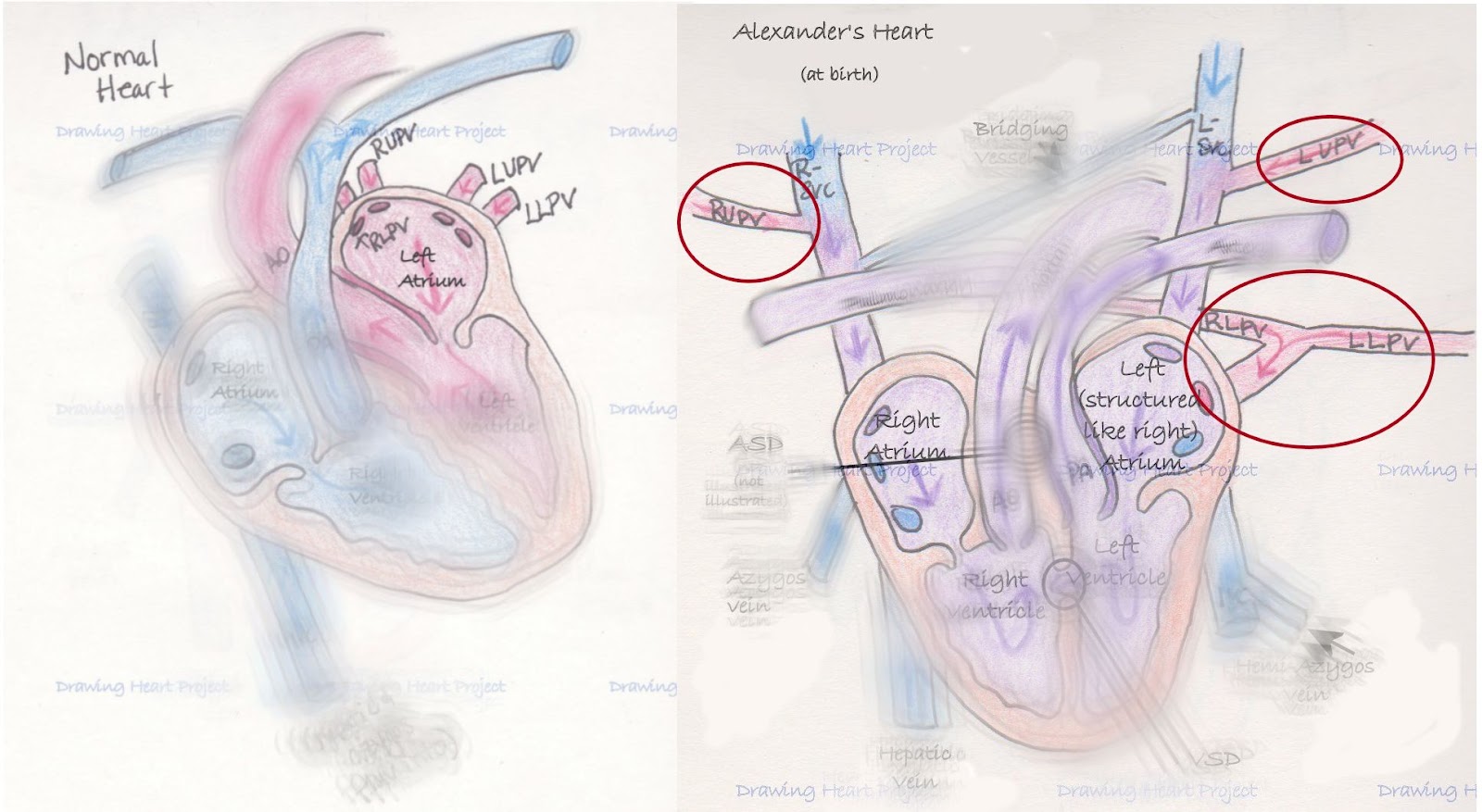
As I’ve described before, in normal anatomy one superior vena cava (SVC)
drains the blood from the upper part of the body directly to the heart. Alexander was born with one on each side of
his body draining to each side of his heart.
He possesses a small bridging vessel between the two and surgeons
elected to utilize that vein to promote better circulation. Just below the bridging vessel, his l-SVC was
tied off and severed, forcing the blood to cross the bridging vessel into the
right SVC and into the right atrium.
This also left his Left Upper Pulmonary Vein (LUPV) to return blood back
to the left side of his heart as it should.

Ventricular defects significantly affect the hemodynamics
(blood flow patterns) inside the heart.
More or less blood flowing into the ventricles significantly change how
well the muscle and valves perform. To
help mitigate the affect, doctors attempted to close a VSD in the heart
wall. The procedure was carried out
well, but more defect remained for repair later.

Finally, surgeons performed an atrial septoctomy. Because of his unique circulation, doctors felt
that having the left and right atrium opened to each other to allow blood to
mix more efficiently. The surgeons
removed the wall separating the left and right atria to create a large atrial
septal defect (ASD) or a surgically common atrium.
Alexander emerged from surgery and was stabilized in the
Cardiac Intensive Care Unit. His chest
was left open to allow for swelling and he remained intubated (as you can’t
draw in breath independently while your sternum is split open.) It was both frightening and reassuring to
watch his tiny heart beat under a thin dressing. His first hours were rocky, but not
unexpected. Four days later his chest
was closed and two days following he was extubated. This surgery staged us for his repair
happening in April.
After having a few complications in the first weeks, Alexander recovered well. His current oxygen saturations are in the low 90s and he is just beginning to show us signs that his heart is holding him back. We feel the timing of this surgery cannot be better. He is strong, yet appearing to plateau. Hopefully this means he'll have a wonderful recovery.
In the next few days, I plan on explaining the next repair Alexander needs for his special heart.
***I am not a nurse or
doctor, nor have I received any formal medical training. Any and all
medical related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the
culmination of countless hours of independent research and medical consultation
and is meant only to communicate my understanding of Alexander’s
condition. It is not intended as medical advice. As always, seek
the advice of a qualified medical professional to explain your specific
diagnosis.***