Because Alexander’s heart is complicated and I am wordy, I
couldn’t quite keep the discussion about his heart in one post. Drawing his heart, his anatomy, his condition
has become very important to me. I
remember those first days when I was searching the web for “heterotaxy
syndrome” and how little information would pop up. I recall that most the articles were
pitifully short and lacking details, or so in-depth I felt I needed a medical
dictionary just to wade through the first paragraph. Little more than a year later, that has
changed for the better, and I want to continue the trend. I want families to be able to understand
Alexander’s diagnoses, and perhaps that would help them understand the ones
they have been presented.
Two Right Atria
The right atrium and the left atrium are structurally
different. They are intended to match
with their corresponding ventricle. For
instance, the electrical impulses that tell the heart to beat originate in the
right, and the left side of the heart is higher pressure system. In Alexander’s heart, the atrium on the left
side of his body is structured like a right atrium. Many doctors say this shouldn’t cause a
problem; if he had two left, he might need a pacemaker. However, it is something of concern to
me. Alexander is unusual that he will
have a two ventricle repair. Not many
heterotaxy-RAI patients are so lucky.
But what is luck for his ventricles, there really is a lack of information
on how well his left-sided atrium will hold up.
Atrial Septal Defect
(ASD) and Ventricular Septal Defect
(VSD)
The separating wall between the left and right side of the
heart is known as the septum. It is
solid and keeps the blue blood from mixing with the red. In utero, there is a small hole (foramen
ovale) between the left and right atrium, but like the ductus arteriosis (DA)
it closes soon after birth. In
Alexander’s case, it was larger than normal and did not close on its own. Alexander also had a moderate sized hole
between his left and right ventricles.
Sometimes these defects close on their own, but Alexander’s were
considered to be too large for that to happen.

Left-sided Inferior
Vena Cava (IVC)
There have been many times when I have been baffled by
Alexander’s anatomy, but none surprises me as much as this defect. The IVC is a right-sided structure. It brings all the deoxygenated blood back to
the heart from the lower part of the body.
It forms from the two iliac veins (one from each leg) and travels just
right of the spine to the right atrium.
All of the lower body’s veins flow into it as it climbs upward. Before entering the atrium, the hepatic veins
from the liver flow into the IVC.

Alexander’s IVC is much different. He has a true left-IVC. It is to the left of the Aorta and spine, and
both of the iliac veins flow into it. It
continues past the renal (kidney) level and flows along what is referred to as
a hemi-azygos continuation. It then
flows into the left side of the heart with no interruptions. Alexander’s hepatic vein connects directly to
the right atrium and his azygos vein connects to the right atrium instead of
the SVC. If you look at the vascular
structure of Alexander’s heart with little regard for labels, you can see how
much the left mirrors the right. While
this anomaly by itself may not cause issue, the flow from the IVC must be
routed back to the proper side of the heart and any surgeon that may operate on
him need to know of his abnormal vasculature to avoid mistakes.

Partial Anomalous
Pulmonary Venous Return (PAPVR)
The pulmonary veins bring oxygen rich blood back to the
heart to be delivered to the body. Each
pulmonary vein (there are typically four, but can be more) independently
attaches to the left atrium.
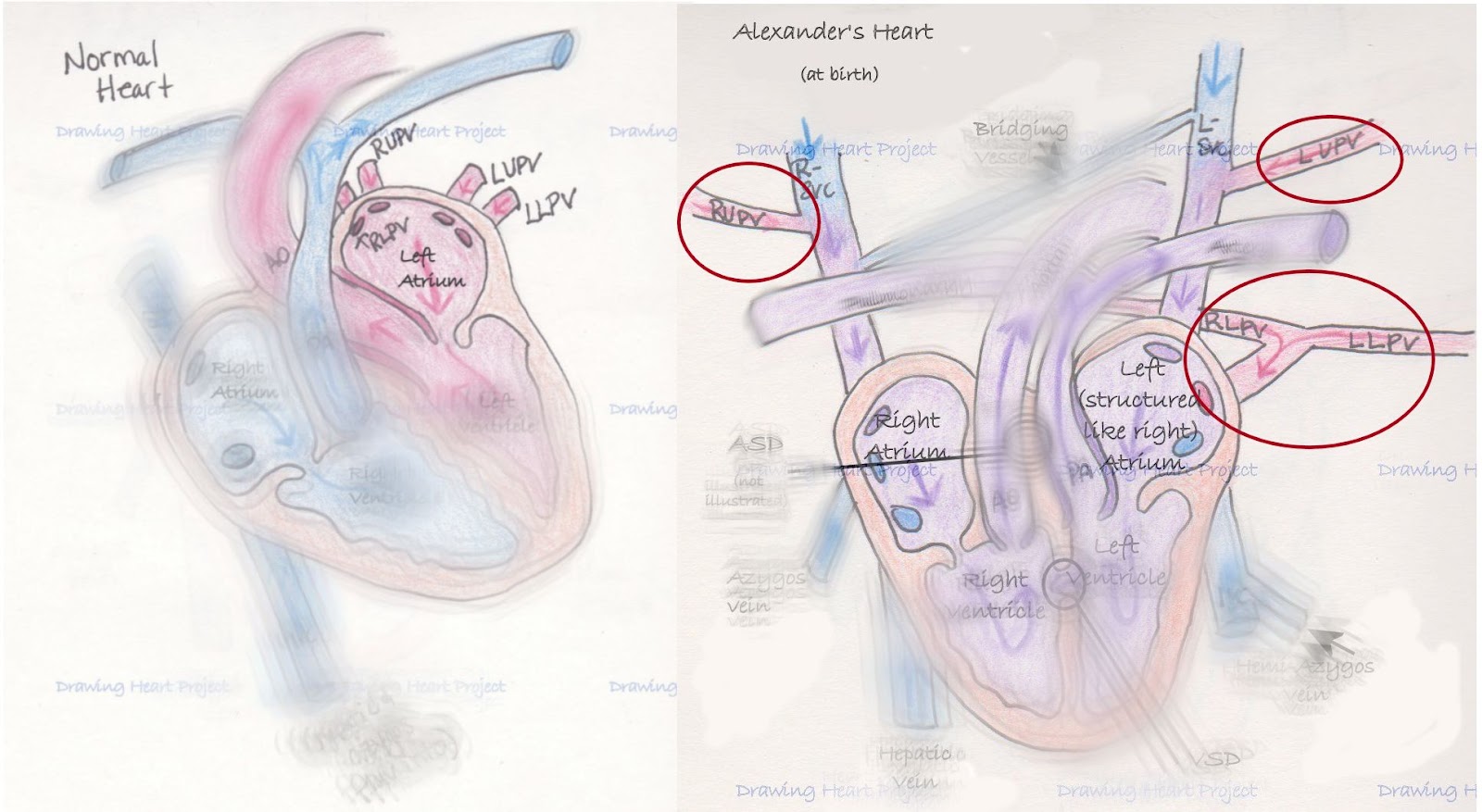
In Alexander’s anatomy, none of his pulmonary veins attach
like they typically should. However,
three of four veins do drain into the left atrium. His right lower pulmonary vein (RLPV) and
left lower pulmonary vein (LLPV) come together in what is known as a confluence
before draining into the left atrium.
The left upper pulmonary vein (LUPV) drains into the L-SVC which drains
to the left atrium. The right upper
pulmonary vein (RUPV) is the problematic one.
It drains into the R-SVC which drains into the right atrium. In a heart with all of its flow being normal,
this would reduce the oxygenated blood around 25%. It also causes an increased workload on the
right ventricle by adding additional blood volume.
Alexander arrived with a special kind of heart. He has certainly had his cardiac team on
their toes learning about his system.
But Alexander has other anomalies, too.
The effects of heterotaxy are far and wide on his tiny system, as is
usual with those with this condition.
His body is like a tiny puzzle, every piece must be scrutinized and fit
together exactly right to function well.
I hope that in my next post I can describe heterotaxy on
more of a broad scale, helping others understand the scope of this terrible
condition.
***I am not a nurse or
doctor, nor have I received any formal medical training. Any and all
medical related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the
culmination of countless hours of independent research and medical consultation
and is meant only to communicate my understanding of Alexander’s
condition. It is not intended as medical advice. As always, seek
the advice of a qualified medical professional to explain your specific
diagnosis.***






