
Monday, November 26, 2012
Intermission
Sunday, October 7, 2012
Heterotaxy RAI vs LAI
(While reading this entry, please remember I am not a medical professional. Also keep in mind that heterotaxy is as different as every patient. Some individuals may have all the conditions described, or very few. This is just a guide for basic understanding.)
I felt like I should bring in a special guest illustrator
for this post. Maybe I was a bit
ambitious, but I enjoy giving others a chance, especially when the artist has
life-long experience with heterotaxy. At
first he was eager, quickly sketching how the internal organs might look, he
was very intense.

Then, he went all “diva” on me, demanded breastmilk, a
cookie and a nap, whining something that sounded a lot like “I can’t possibly
work under these deplorable conditions”.
Of course, I was forced to tuck 16 month old Alexander into his bed and
go on without him, even though I think there may be some degree of accuracy to
his unfinished drawing.
Humor aside, there are days when his scribbles make me think
of heterotaxy. The literal translation
of heterotaxy is “different arrangement”.
There is not a consensus on exactly how that applies, but many feel that
the heart is always involved (though, perhaps not to a great degree), and there
is some abdominal ambiguity.
Looking at a person from the outside, it’s hard to imagine
the complexity that lies on the inside.
Generally speaking, the outside appearance of a person is symmetrical
between the left and right side. A
person’s arms are about the same size and length, their feet are about the same
size, and the ears are near the same spot.
The left side is much like a mirror image of the right, or vise versa.
On the inside it’s the opposite. The left side is completely different from
the right. The stomach is on the left
side of the body, the liver on the right.
Even paired organs that have one organ on each side of the body are
structurally different from each other.
For instance the left lung only has two lobes, while the right has three
and the right adrenal gland is triangular shaped and the left horseshoe shaped.



Heterotaxy disrupts this asymmetrical balance. During the early days of a pregnancy (between
the 3rd and 6th week) the internal organs are
forming. They are created from tubes of
tissue that are told how to twist and turn to form the intricate chambers of
the heart, blood vessels and digestive tract.
In heterotaxy, these twists and turns don’t happen the way they should,
and it’s not entirely understood why.
There are some genetic markers that indicate inherited heterotaxy, and
sometimes the syndrome does run in families.
There is also some evidence that heterotaxy (whole or in part) could be
related to Primary Ciliary Dyskensia (PCD) which affects the ability of tiny
hairs (cilia) in our bodies to move things around they way they should.

Most cases of heterotaxy can be organized into two
types. There is Left Atrial Isomerism
(LAI) and Right Atrial Isomerism (RAI).
To better understand what is happening, it helps to know the definition
of isomerism. Isomerism is a chemistry
term that describes different compounds that are made up of the same parts
(atoms), but they are bonded together differently, and that makes the compound
completely different. The use of
isomerism when referring to heterotaxy describes optical isomerism, or when
those compounds are arranged in such a way they are the mirror images of the
other.
Remembering from earlier, think of the outside of our body
as optically isomeric; it is made up of the same parts, but in a mirror image
to the other. However, the inside isn’t
supposed to be, as there are drastic differences between the right and left
internal organs. Therefore, in RAI, all the parts of the right side are
present, but mirror imaged to the left, and in LAI all of the left-sided
structures are there, but mirror imaged to the right. This isn’t perfect, but it does help when
knowing what to expect from a RAI patient versus a LAI.

In RAI, the structures of the heart are usually greatly
affected. Much of the heart lies on the
left side of our bodies, so it makes sense that when the right side of the body
is copied, the heart would suffer. The
lungs often end up as two tri-lobed lungs (as the right lung is tri-lobed), the
stomach is on the right side of the body versus the left, the spleen is
generally absent (asplenia). The liver
usually becomes transverse (midline) and the gall bladder can be affected, and
the intestines are often malrotated and the kidneys and adrenal glands can
suffer some anomalies.

In LAI one can almost infer the opposite to be true. The heart tends to have less structural
problems, but more prone to electrical ones as the heart’s natural pacemaker is
located in the right atrium. Often, the
lungs are both bi-lobed (and bi-lobed lungs are slightly smaller than
tri-lobed). The liver can be midline and
malrotated intestines might be present.
Many patients have polysplenia (or many spleens), and while one may
think many is much better than none, often times they are not working. This is known as functional asplenia. Differences can also affect the kidneys and
adrenals.
Because of how complex and extensive this syndrome is, every
person affected is different. One could
talk to twenty patients and their families and hear twenty different stories
and diagnoses. These families have teams
of doctors to help keep their children in the best possible health. Our family has been fortunate that Alexander
has been so well, but we’re also aware that the luck may not hold out
forever. Our hope is to continue to
bring attention to this rare congenital syndrome. Only through awareness can we convince people
to care, and when enough people care change can happen.
I am not a nurse or doctor, nor have I received any formal
medical training. Any and all medical
related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the culmination of
countless hours of independent research and medical consultation and is meant
only to communicate my understanding of Alexander’s condition. It is not intended as medical advice. As always, seek the advice of a qualified
medical professional to explain your specific diagnosis.
Wednesday, September 19, 2012
Differences part 2
Because Alexander’s heart is complicated and I am wordy, I
couldn’t quite keep the discussion about his heart in one post. Drawing his heart, his anatomy, his condition
has become very important to me. I
remember those first days when I was searching the web for “heterotaxy
syndrome” and how little information would pop up. I recall that most the articles were
pitifully short and lacking details, or so in-depth I felt I needed a medical
dictionary just to wade through the first paragraph. Little more than a year later, that has
changed for the better, and I want to continue the trend. I want families to be able to understand
Alexander’s diagnoses, and perhaps that would help them understand the ones
they have been presented.
Two Right Atria
The right atrium and the left atrium are structurally
different. They are intended to match
with their corresponding ventricle. For
instance, the electrical impulses that tell the heart to beat originate in the
right, and the left side of the heart is higher pressure system. In Alexander’s heart, the atrium on the left
side of his body is structured like a right atrium. Many doctors say this shouldn’t cause a
problem; if he had two left, he might need a pacemaker. However, it is something of concern to
me. Alexander is unusual that he will
have a two ventricle repair. Not many
heterotaxy-RAI patients are so lucky.
But what is luck for his ventricles, there really is a lack of information
on how well his left-sided atrium will hold up.
Atrial Septal Defect
(ASD) and Ventricular Septal Defect
(VSD)
The separating wall between the left and right side of the
heart is known as the septum. It is
solid and keeps the blue blood from mixing with the red. In utero, there is a small hole (foramen
ovale) between the left and right atrium, but like the ductus arteriosis (DA)
it closes soon after birth. In
Alexander’s case, it was larger than normal and did not close on its own. Alexander also had a moderate sized hole
between his left and right ventricles.
Sometimes these defects close on their own, but Alexander’s were
considered to be too large for that to happen.

Left-sided Inferior
Vena Cava (IVC)
There have been many times when I have been baffled by
Alexander’s anatomy, but none surprises me as much as this defect. The IVC is a right-sided structure. It brings all the deoxygenated blood back to
the heart from the lower part of the body.
It forms from the two iliac veins (one from each leg) and travels just
right of the spine to the right atrium.
All of the lower body’s veins flow into it as it climbs upward. Before entering the atrium, the hepatic veins
from the liver flow into the IVC.

Alexander’s IVC is much different. He has a true left-IVC. It is to the left of the Aorta and spine, and
both of the iliac veins flow into it. It
continues past the renal (kidney) level and flows along what is referred to as
a hemi-azygos continuation. It then
flows into the left side of the heart with no interruptions. Alexander’s hepatic vein connects directly to
the right atrium and his azygos vein connects to the right atrium instead of
the SVC. If you look at the vascular
structure of Alexander’s heart with little regard for labels, you can see how
much the left mirrors the right. While
this anomaly by itself may not cause issue, the flow from the IVC must be
routed back to the proper side of the heart and any surgeon that may operate on
him need to know of his abnormal vasculature to avoid mistakes.

Partial Anomalous
Pulmonary Venous Return (PAPVR)
The pulmonary veins bring oxygen rich blood back to the
heart to be delivered to the body. Each
pulmonary vein (there are typically four, but can be more) independently
attaches to the left atrium.
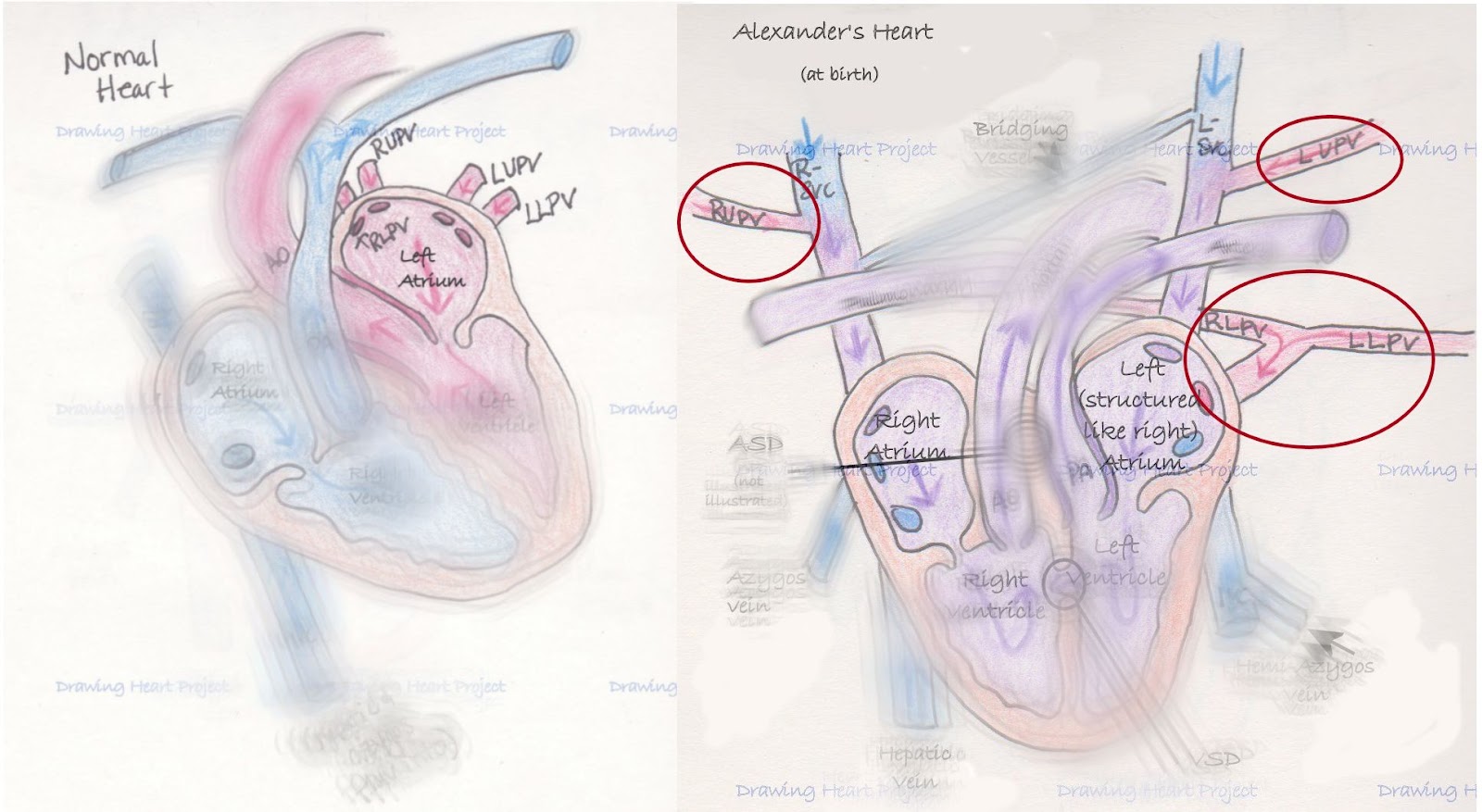
In Alexander’s anatomy, none of his pulmonary veins attach
like they typically should. However,
three of four veins do drain into the left atrium. His right lower pulmonary vein (RLPV) and
left lower pulmonary vein (LLPV) come together in what is known as a confluence
before draining into the left atrium.
The left upper pulmonary vein (LUPV) drains into the L-SVC which drains
to the left atrium. The right upper
pulmonary vein (RUPV) is the problematic one.
It drains into the R-SVC which drains into the right atrium. In a heart with all of its flow being normal,
this would reduce the oxygenated blood around 25%. It also causes an increased workload on the
right ventricle by adding additional blood volume.
Alexander arrived with a special kind of heart. He has certainly had his cardiac team on
their toes learning about his system.
But Alexander has other anomalies, too.
The effects of heterotaxy are far and wide on his tiny system, as is
usual with those with this condition.
His body is like a tiny puzzle, every piece must be scrutinized and fit
together exactly right to function well.
I hope that in my next post I can describe heterotaxy on
more of a broad scale, helping others understand the scope of this terrible
condition.
***I am not a nurse or
doctor, nor have I received any formal medical training. Any and all
medical related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the
culmination of countless hours of independent research and medical consultation
and is meant only to communicate my understanding of Alexander’s
condition. It is not intended as medical advice. As always, seek
the advice of a qualified medical professional to explain your specific
diagnosis.***
Friday, September 14, 2012
Differences

Even with no knowledge of heart conditions, it’s easy to see
Alexander’s heart is significantly different from a normal one. It was created uniquely, just inside his tiny
body and no where else. However, it has
and continues to work for him. He’s a
special heterotaxy-RAI guy that’s fortunate enough to have two ventricles. The following is how I perceive his
differences. Please remember, I’m just a
mom devouring medical documents, not a trained medical professional.
Dextrocardia (Incomplete)
Dextrocardia is when the heart is on the opposite side of
the body. Normally the human heart is
located just on the left side of the body with the apex the furthest point
left. Oddly enough, the apex is not at
the top of the heart, but the very bottom.
In complete dextrocardia, the heart is just on the right side, with the
apex furthest right. It would look
something like this:

Alexander’s dextrocardia is incomplete. His heart is completely midline, straight as
you are looking at him, with the apex of his heart near the tip of his sternum.

While in itself, this is not a problem, it has many
effects. It makes surgery more
difficult, as the parts and structures surgeons are familiar with are not where
they normally are, and creates new problems when trying to re-route heart
plumbing. It makes it more difficult to
get accurate readings with ECG (electrocardiogram), it makes Echos
(echocardiograms/ultrasound of the heart) harder to read. Most of all, it’s indicative of other
structural differences of the heart.
dextro-Transposition of the Great Arteries (d-TGA)
d-TGA generally happens when the heart is forming, near the
24th day of pregnancy.
Instead of twisting one last time, the Aorta and Pulmonary Artery remain
parallel to one another. While mother is
carrying the baby, it has no effect, as the mother oxygenates the blood (baby
doesn’t breathe) and the Aorta and Pulmonary Artery are connected by the Ductus
Arteriosis (DA). For such a simple
problem, it devastates the circulatory system.

At birth, a mother’s hormones stop being passed to baby and
the DA begins to close. The body gets
less and less oxygen. In d-TGA, instead
of operating as an entire system, the heart operates as two closed loops. The blue blood enters the heart on the right
side and is immediately sent back out to the body through the Aorta. On the left, blood rich in oxygen from the
lungs enters the left and is sent directly back to the lungs. The result is the body’s tissues are never
oxygenated and the lungs receive blood at high pressure. Without surgery, death is near certain by one
year of age.
While Alexander was born with this condition, because of his
other defects, d-TGA was not able to leave his body with no oxygen.
Dual Superior Vena Cava
(SVC)
Because of Alexander’s heterotaxy, many structures that
normally occur on the right are copied onto the left. The SVC is the major vessel that drains all
of the blood from the upper part of the body (from the heart up) back to the
heart so it can be re-oxygenated. It
connects to the right atrium.

Alexander also has one on his left side. It connects into the left atrium much like
the other side. There was one small
bridging vessel between the right and left SVCs. The left SVC is problematic because it would
return blue blood to the side of the heart that deals with red. Instead of being able to head to the lungs
and exchange its carbon dioxide for oxygen, it would simply mix with red blood
and head out to the body.
Those are three of Alexander’s heart defects; he has five
others. Like all of his heterotaxy brothers
and sisters, his anatomy is complicated.
In the interest of keeping blog sizes manageable, I’ll save those for
later.
***I am not a nurse or doctor, nor have I received any formal
medical training. Any and all medical
related information on Alexander’s Fight is the product of a mother’s
desperation to understand and advocate for her child. This series of notes is the culmination of
countless hours of independent research and medical consultation and is meant
only to communicate my understanding of Alexander’s condition. It is not intended as medical advice. As always, seek the advice of a qualified
medical professional to explain your specific diagnosis.***
Sunday, September 9, 2012
A Normal Heart

When I began my journey understanding Alexander's heart, I realized that I must know what a regular heart does and looks like. Only then, could I appreciate the special structures, the innovative compensation, and unique organ my son possesses in his chest. It simply amazes me how a body can learn to deal with adversity and just how strong the body's instinct to survive is.
The heart is a miraculous machine. It’s a pump that circulates blood throughout
our bodies. It delivers oxygen and
nutrients to our tissues and disposes of the carbon dioxide and other
waste. It pumps approximately 60 times
per minute, every minute of every day.
In a 50 year lifespan that’s approximately 1,576,800,000 times. Yes, about one and a half BILLION times.
In a normal heart, blood enters from the body through veins on
the right side. Its oxygen stores are
depleted and it’s blue. It’s received in
the right atrium, passes through the tricuspid valve into the right ventricle
so it can head to the lungs. When the
right ventricle squeezes, it leaves through the pulmonary valve in the
pulmonary artery.
The pulmonary artery branches and delivers blood to both
lungs. Here, the carbon dioxide waste is
traded for oxygen and the blood is red again.
It returns to the heart through the pulmonary veins (there are usually 4
of these, but more can occur naturally) into the left atrium. When the heart relaxes, the oxygenated blood
passes through the bicuspid (or mitral) valve into the left ventricle. With the next pump of the heart, the blood is
pushed out of the aorta, through the aortic valve where it travels to the body
to deliver its oxygen and nutrients.
This is a very elegant solution that supports every system
in our body. And every year 1 out of
every 100 children born will have one that is less than perfect. Congenital Heart Disease (CHD) claims more
lives than all of childhood cancers combined and is the leading cause of death
in children. Our children need us to
understand how this miraculous muscle works.
Alexander has no less than eight CHDs. Less than 10 years ago, his diagnosis (Heterotaxy-Right Atrial Isomerism) had 80% mortality before the first birthday. While the numbers are improving today, they still are frighteningly poor. It is a constant worry, but odds we plan on defeating.
This is Alexander's heart beside a normal one. It's obvious that it's different, but it's still strong. His specific heart diagnoses are:
Dextrocardia (not complete)
d-TGA (dextro-Transposition of the Great Arteries)
Dual SVC
two right atria
ASD (Atrial Septal Defect)
VSD (Ventricular Septal Defect)
left-sided IVC
PAPVR (Partial Anomalous Pulmonary Venous Return)
Among children born with Heterotaxy-RAI, he is lucky. His left ventricle is full size and fully functioning. He lacked defects involving his pulmonary and aortic valves and it's hopeful that we can straighten out his circulatory system without compromising his quality of life. We are hopeful and he is strong.
Dextrocardia (not complete)
d-TGA (dextro-Transposition of the Great Arteries)
Dual SVC
two right atria
ASD (Atrial Septal Defect)
VSD (Ventricular Septal Defect)
left-sided IVC
PAPVR (Partial Anomalous Pulmonary Venous Return)
Among children born with Heterotaxy-RAI, he is lucky. His left ventricle is full size and fully functioning. He lacked defects involving his pulmonary and aortic valves and it's hopeful that we can straighten out his circulatory system without compromising his quality of life. We are hopeful and he is strong.
***I am not a nurse or doctor, nor have I received any formal
medical training. Any and all medical
related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the culmination of
countless hours of independent research and medical consultation and is meant
only to communicate my understanding of Alexander’s condition. It is not intended as medical advice. As always, seek the advice of a qualified
medical professional to explain your specific diagnosis.***
Saturday, September 8, 2012
Drawing Heart
***I am not a nurse or doctor, nor have I received any formal
medical training. Any and all medical
related information on Drawing Heart Project is the product of a mother’s
desperation to understand and advocate for her child. This blog is the culmination of
countless hours of independent research and medical consultation and is meant
only to communicate my understanding of Alexander’s condition. It is not intended as medical advice. As always, seek the advice of a qualified
medical professional to explain your specific diagnosis.***
From the moment Alexander was born he was making doctors ask
questions. Because of fetal imaging we
knew he would be born with d-TGA (dextro-Transposition of the Great
Arteries). Traditionally, these infants
have been called “blue babies” as the circulation did not allow oxygen into
their blood and to their bodies.
Alexander was born pink and continued to be. Doctors knew something else must be occurring
for him to be so well oxygenated.
Within hours, Alexander was the main attraction in the
NICU/CICU. Every doctor came to look at
him, tons of imaging was done, nurses were constantly puzzled about his true
condition. We had one doctor that
consistently drew pictures for the other staff, trying to communicate
Alexander’s entire heart status.
Terminology was constantly thrown out, and Matt and I weren’t nearly as
educated on the topic as we are now.
At eight days old, they prepared to take him into surgery
for the first time. The cardiac surgeon
talked to us about his conditions and the surgical plan when he spoke the words
that inspired this project.
“He’s unique; no other like him. You won’t find a picture of his heart in a
book or online. He’s as rare as they
come.”
That upset me. How
could I, a “normal” parent, understand when the doctors are not only delivering
diagnoses that I’ve never heard of, made up of multiple words that each need a
google search, but have no real illustrations to go with it? How could I grasp Alexander’s entire
condition “blindly?”
The answer was a long amount of time, a ton of research and,
eventually, sketching his anatomy. It
brought a great amount of confidence understanding his condition and being able
to communicate it. I’ve found myself
sketching the same heart pictures over and over, refining them, explaining his
special heart to the newest doctor.
That brings me to now, and the project that’s known as
“Drawing Heart” on my hard disk. I
realized that if I had trouble understanding Alexander’s condition, others must
have as well. I decided that I would
draw the structures and conditions that have become so familiar to me in hope
that others would be able to better understand by looking and reading my own
interpretations. My goal is to raise
awareness and understanding for all things heterotaxy.

For now I’ll just leave my drawing of Alexander’s special
heart when he was born(so now a picture of it can be found online!), but I will explain it in a later post. I hope “Drawing Heart” brings attention and
increases understanding.
Subscribe to:
Posts (Atom)