(While reading this entry, please remember I am not a medical professional. Also keep in mind that heterotaxy is as different as every patient. Some individuals may have all the conditions described, or very few. This is just a guide for basic understanding.)
I felt like I should bring in a special guest illustrator
for this post. Maybe I was a bit
ambitious, but I enjoy giving others a chance, especially when the artist has
life-long experience with heterotaxy. At
first he was eager, quickly sketching how the internal organs might look, he
was very intense.

Then, he went all “diva” on me, demanded breastmilk, a
cookie and a nap, whining something that sounded a lot like “I can’t possibly
work under these deplorable conditions”.
Of course, I was forced to tuck 16 month old Alexander into his bed and
go on without him, even though I think there may be some degree of accuracy to
his unfinished drawing.
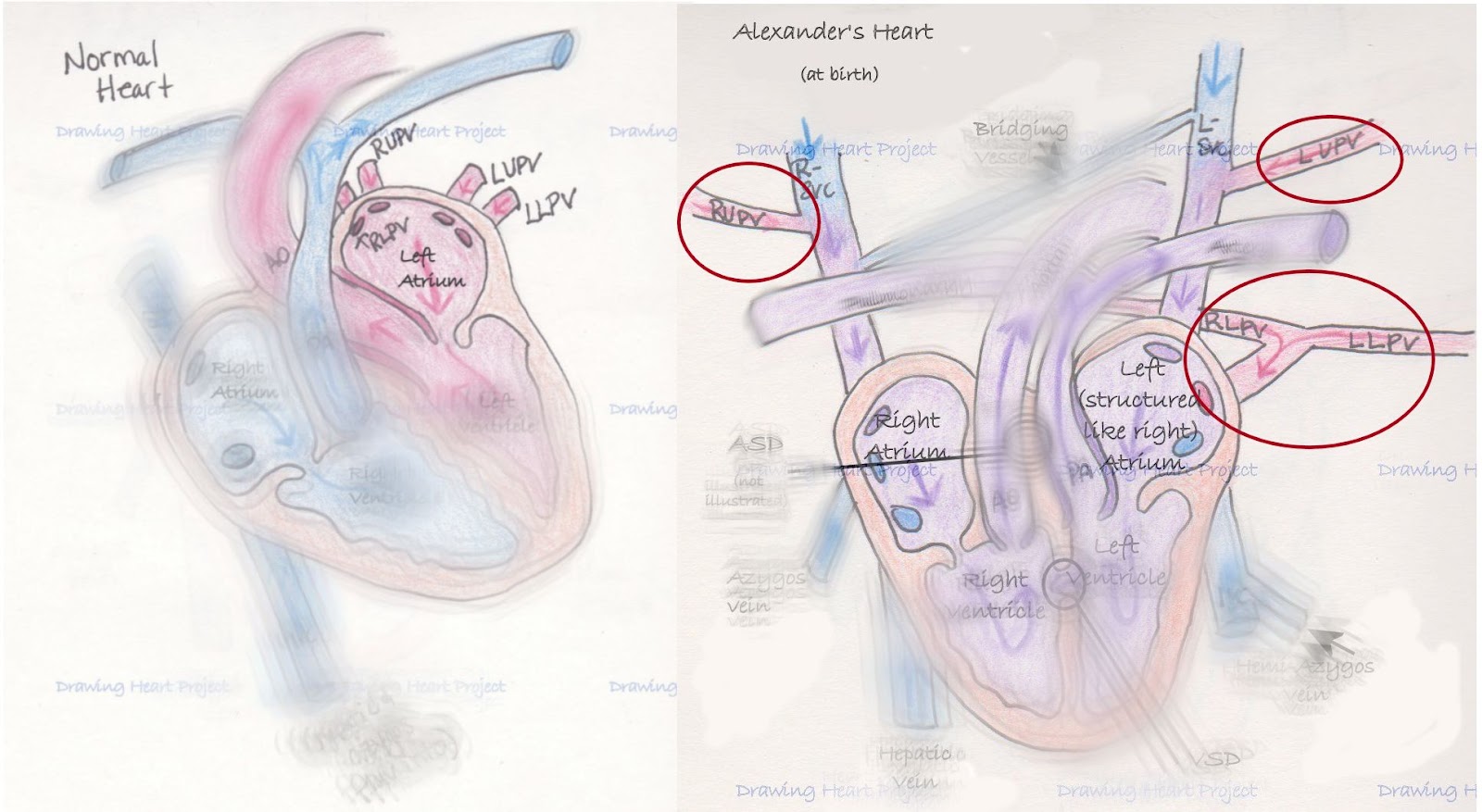
Humor aside, there are days when his scribbles make me think
of heterotaxy. The literal translation
of heterotaxy is “different arrangement”.
There is not a consensus on exactly how that applies, but many feel that
the heart is always involved (though, perhaps not to a great degree), and there
is some abdominal ambiguity.
Looking at a person from the outside, it’s hard to imagine
the complexity that lies on the inside.
Generally speaking, the outside appearance of a person is symmetrical
between the left and right side. A
person’s arms are about the same size and length, their feet are about the same
size, and the ears are near the same spot.
The left side is much like a mirror image of the right, or vise versa.
On the inside it’s the opposite. The left side is completely different from
the right. The stomach is on the left
side of the body, the liver on the right.
Even paired organs that have one organ on each side of the body are
structurally different from each other.
For instance the left lung only has two lobes, while the right has three
and the right adrenal gland is triangular shaped and the left horseshoe shaped.



Heterotaxy disrupts this asymmetrical balance. During the early days of a pregnancy (between
the 3rd and 6th week) the internal organs are
forming. They are created from tubes of
tissue that are told how to twist and turn to form the intricate chambers of
the heart, blood vessels and digestive tract.
In heterotaxy, these twists and turns don’t happen the way they should,
and it’s not entirely understood why.
There are some genetic markers that indicate inherited heterotaxy, and
sometimes the syndrome does run in families.
There is also some evidence that heterotaxy (whole or in part) could be
related to Primary Ciliary Dyskensia (PCD) which affects the ability of tiny
hairs (cilia) in our bodies to move things around they way they should.

Most cases of heterotaxy can be organized into two
types. There is Left Atrial Isomerism
(LAI) and Right Atrial Isomerism (RAI).
To better understand what is happening, it helps to know the definition
of isomerism. Isomerism is a chemistry
term that describes different compounds that are made up of the same parts
(atoms), but they are bonded together differently, and that makes the compound
completely different. The use of
isomerism when referring to heterotaxy describes optical isomerism, or when
those compounds are arranged in such a way they are the mirror images of the
other.
Remembering from earlier, think of the outside of our body
as optically isomeric; it is made up of the same parts, but in a mirror image
to the other. However, the inside isn’t
supposed to be, as there are drastic differences between the right and left
internal organs. Therefore, in RAI, all the parts of the right side are
present, but mirror imaged to the left, and in LAI all of the left-sided
structures are there, but mirror imaged to the right. This isn’t perfect, but it does help when
knowing what to expect from a RAI patient versus a LAI.

In RAI, the structures of the heart are usually greatly
affected. Much of the heart lies on the
left side of our bodies, so it makes sense that when the right side of the body
is copied, the heart would suffer. The
lungs often end up as two tri-lobed lungs (as the right lung is tri-lobed), the
stomach is on the right side of the body versus the left, the spleen is
generally absent (asplenia). The liver
usually becomes transverse (midline) and the gall bladder can be affected, and
the intestines are often malrotated and the kidneys and adrenal glands can
suffer some anomalies.

In LAI one can almost infer the opposite to be true. The heart tends to have less structural
problems, but more prone to electrical ones as the heart’s natural pacemaker is
located in the right atrium. Often, the
lungs are both bi-lobed (and bi-lobed lungs are slightly smaller than
tri-lobed). The liver can be midline and
malrotated intestines might be present.
Many patients have polysplenia (or many spleens), and while one may
think many is much better than none, often times they are not working. This is known as functional asplenia. Differences can also affect the kidneys and
adrenals.
Because of how complex and extensive this syndrome is, every
person affected is different. One could
talk to twenty patients and their families and hear twenty different stories
and diagnoses. These families have teams
of doctors to help keep their children in the best possible health. Our family has been fortunate that Alexander
has been so well, but we’re also aware that the luck may not hold out
forever. Our hope is to continue to
bring attention to this rare congenital syndrome. Only through awareness can we convince people
to care, and when enough people care change can happen.
I am not a nurse or doctor, nor have I received any formal
medical training. Any and all medical
related information on Drawing Heart is the product of a mother’s
desperation to understand and advocate for her child. This blog is the culmination of
countless hours of independent research and medical consultation and is meant
only to communicate my understanding of Alexander’s condition. It is not intended as medical advice. As always, seek the advice of a qualified
medical professional to explain your specific diagnosis.